
Type II hypersensitivity reaction: Mechanism and examples
- Type II hypersensitivity reaction involves antibody mediated destruction of cells. It is also known as cytotoxic reaction.
- In this hypersensitivity reaction, specific antibody (IgG or IgM) bound to cell surface antigen and destroy the cell. If the cell is microorganism, killing of cell is beneficial to host. However in Type II hypersensitivity, the cells are own RBC.
- The killing of cell can occurs by one of the three mechanisms. They are-
- Complement mediated cell lysis
- Antibody dependent cell mediated cytotoxicity (ADCC)
- Opsonization
1. Complement mediated lysis of cell:
- Complement system is a system of lytic enzyme which are usually inactive in blood.
- Enzymes of complement system are activated by antigen-antibody complex.
- When antibody binds to antigen (microorganism or RBC) they form Ag-ab complex.
- Ag-ab complex can activate complement system by three different mechanism-classical pathway, alternate pathway and lectin pathway.
- Activated complement proceeds in cascade mechanism.
- When complement is activated on the surface of cell (RBC) it causes lysis of cell.
2. Antibody dependent cell mediated cytotoxicity (ADCC):
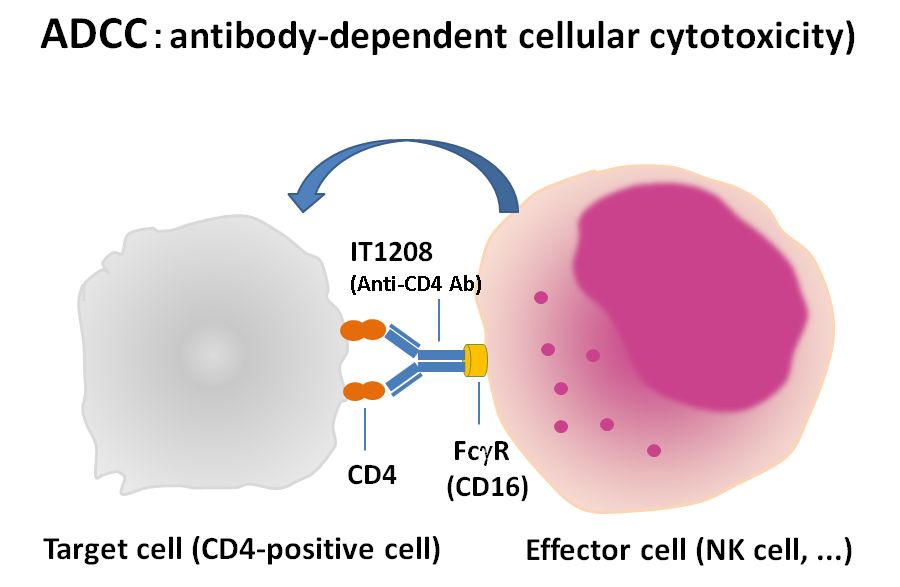
- Antibody binds with antigen by its Fab portion. However Fc region of antibody has receptor on cytotoxic cells. So, antibody cross link target cell (microorganism or RBC) with cytotoxic cells and promote killing.
- Most cytotoxic cells contain storage of hydrolytic and digestive enzymes. These enzymes are released on the surface of target cell (MOs or RB or target cell), killing them.
- Here antibody itself does not kill or destroy cell but rather mediate killing by presenting antigen to cytotoxic cell. Similarly cytotoxic cell depends upon antibody to bind antigen. So this mechanism is known as Antibody dependent cell mediated cytotoxicity.
3. Opsonization:
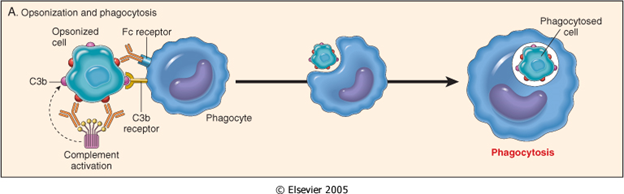
- When antigen enters into host body, antibodies are produced.
- Antibody binds to antigen through Fab region. Fc region of antibody remains free.
- Phagocytic cells such as Neutrophils, macrophages and monocytes have receptors that can bind to Fc region of antibody. The receptor is known as FcR.
- In this case antibody molecule directly cross links antigen (Microrganism or RBC or target cell) with phagocytic cells. This cross-linkage activates phagocytic cells and increases the rate of phagocytosis.
- This increased rate of phagocytosis by binding of antibody to antigen is called Opsonization.
Some examples of Type II hypersensitivity reaction:
1. Blood transfusion reaction:
- ABO blood transfusion reaction is an example of type II hypersensitivity reaction. Human RBCs contains A and/or B antigen as major antigen on the surface of RBC. Other minor antigens such as Rh, Kell, Duffy etc are also present. Antibodies to ABO antigen are called isohemagglutinin and are usually of IgM class whereas antibodies to other minor antigen are of IgG class.
- An individual with blood group A recognizes B antigen like epitope (blood group B) as foreign and produces isohemagglutinin (antibodies). The same individual does not produce antibodies to A antigen as it is similar to self antigen, so that state of tolerance exists.
- If individual with blood group A is transfused with blood containing B antigen then transfusion reaction occurs in which anti-B isohemagglutinin ( antibodies) binds with B- blood cells and mediate destruction of transfused RBC by complement activation.
- Since lysis of RBC occurs in intravascular space, free hemoglobin appears in urine. Hemoglobin may be converted into billirubin which is highly toxic to tissues.
- For treatment of this hypersensitivity reaction, transfusion should be stopped immediately. Furthermore patients should be given diuretic to eliminate hemoglobin in urine.
- Blood transfusion reaction occurs immediately in case of mismatched ABO antigen. In this case transfused RBCs are lysed by complement.
- In case of minor antigen (Rh) mismatched, delayed reaction occurs and in this case transfused RBCs are lysed by opsonization (IgG antibody) and no free hemoglobin appears in urine.
2. Hemolytic disease of new born (Erythroblastosis fetalis):
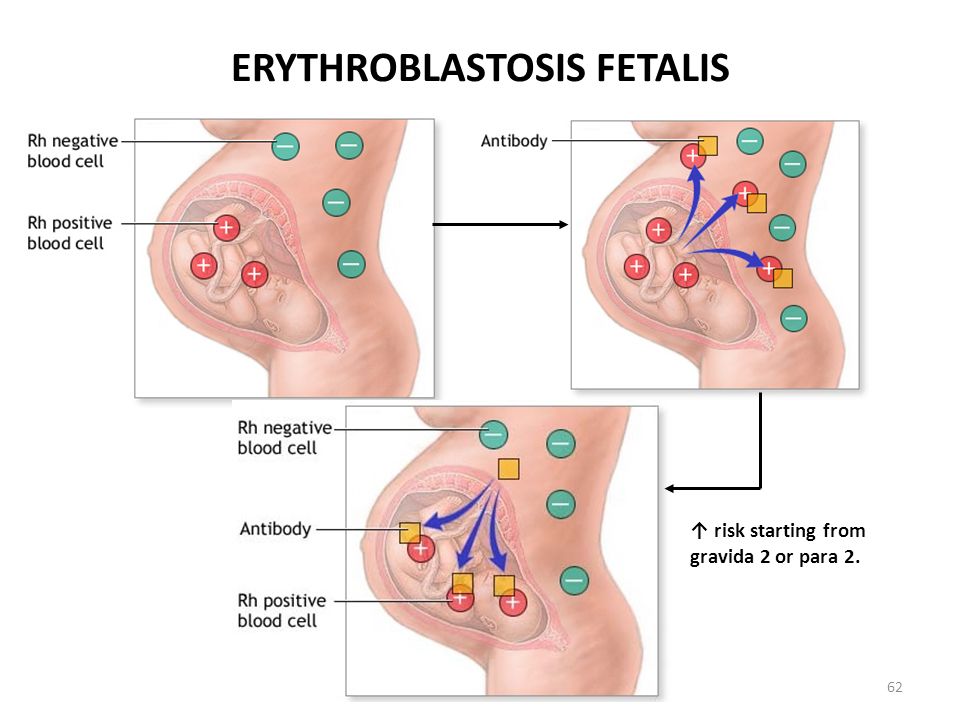
- Hemolytic disease of newborn develops when maternal IgG antibodies specific for fetal blood group crosses placenta and destroy fetal RBCs.
- The consequences of such transfer of antibody can be minor, serious or lethal to fetus.
- Serious hemolytic diseases of new born develops when Rh –ve mother conceive Rh +ve fetus, which causes erythroblastosis fetalis.
- During pregnancy fetal RBCs are separated from mother’s circulation by a layer of cell in placenta called trophoblast. During her 1st pregnancy with Rh+ve fetus, mother circulation is not exposed to enough fetal RBC to activate Rh specific B cells for antibody production.
- At the time of delivery, large amount of fetal umbilical cord blood enter to mother’s circulation. These fetal blood activates mother Rh specific B cells resulting in production of plasma cell and memory cell. The plasma cell produce IgM antibodies which binds and destroy fetal RBCs from mother’s circulation but the memory cell remains which threat any subsequent pregnancy with Rh+ve fetus.
- Activation of memory cells in subsequent pregnancy with Rh+ve fetus causes production of IgG antibodies which can cross placenta and destroy fetal RBCs.
- Mild to severe anemia develops in fetus and sometime fetal. The conversion of hemoglobin to billirubin produces additional threat to new born because billirubin may accumulate in brain and damage it.
- This hemolytic disease of new born can be prevented by injecting preformed antibodies against Rh antigen to mother at around 28 weeks of pregnancy and within 24-48 hours of 1st The antibodies marketed as Rhogam. These antibodies bind to RBCs of fetus in mother circulation and clear before B cell activation.
3. Drug induced hemolytic anemia:
- Certain drugs such as penicillin, cephalosporin and streptomycin can absorb non-specifically to protein on surface of RBC forming complex similar to hepten-carrier complex.
- In some patients these complex induce formation of antibodies, which binds to drugs on RBC and induce complement mediated lysis of RBC and thus produce progressive anemia.
- This drug induced hemolytic anemia is an example of Type II hypersensitivity reaction.
Type II hypersensitivity reaction: Mechanism and examples