
Plasmodium falciparum: morphology, life cycle, pathogenesis and clinical disease
- Plasmodium falciparum is the most virulent species of Plasmodium in human. It causes malignant tertian or falciparum malaria. The name ‘falciparum’ is derived by Welch from ‘falx’ meaning sickle or crescent and ‘parere’ meaning to bring forth.
Habitat:
- Various stages of malarial parasites are found inside the parenchymal cellsof liver and inside RBCs of Human.
Morphology:
Following are the diagnostic forms of parasite found in human
-
Ring form:
- This is the young trophozoite found inside RBCs. The name ring is derived from the morphological appearance of the stage resembling a ring like structure.
- It consists of central vacuole and nucleus present at the center in the cytoplasm. Often two or more rings forms of the parasite are found inside a single RBC.
- In stained smear, ring shaped cytoplasm surrounds central blue colored vacuole with red colored nucleus on it.
-
Trophozoites:
- The trophoizoites ae vacuolated more or less amoeboid and uninucleated.
- They are small, delicate and measures 1.25 -1.5 µm in size
- In a stained preparation, they show a thin ring of blue cytoplasm and darkish stained nucleus.
- In heavy infection, growing forms assume the shape of compact form.
- Single large mass of pigment colored yellow to black called haemozoin are present.
-
Schizonts:
- They are small, immobile, asexual and dividing form of parasite.
- They measure 4.5-5 µm in diameter and occupy about 2/3rd of the infected RBC.
- Each schizont contains two or four merozoites and an aggregate of dark stained pigments
- On maturation schizont contains 10-36 merozoites arranged in grape like cluster.
- Each merozoite measure 5-10µm in length.
- Schizonts are very rarely seen in peripheral blood smear. Presence of schizonts in peripheral blood suggests severe infection.
-
Gametocytes:
- Gametocytes are sexual and erythrocytic stage of parasite and are infectious to mosquitoes.
- They are typically crescent (banana) shape with round or pointed ends.
- Size of mature gametocyte is about one and half time larger than RBC.
- There are two types of gametocytes.
- Microgamete: male form
- Macrogamete: female form
-
Sporozoites:
- The sporozoites are the infective form and are infectious to human
- They are found in infected mosquitoes.
- Sporozoites are single nucleated, sickled shaped structure with equally pointed ends. They have complex structure and a thick pellicle.
- Pellicle consists of a thin outer membrane, a two layered membrane and a layer of subpericular microtubules. They contain 3 polar rings and a mitochondrion present at posterior end.
- The peripheral fibres serves as organ of locomotion.
- They measures 10-15 µm in length
-
Ookinete and Oocyst:
- They are other form found in infected mosquitoes.
Life cycle of Plasmodium falciparum:
- Malaria parasite shows alternation of generation with alternation of hosts.
- Intermediate host (Human): asexual cycle take place
- Definitive host (mosquito): sexual cycle take place
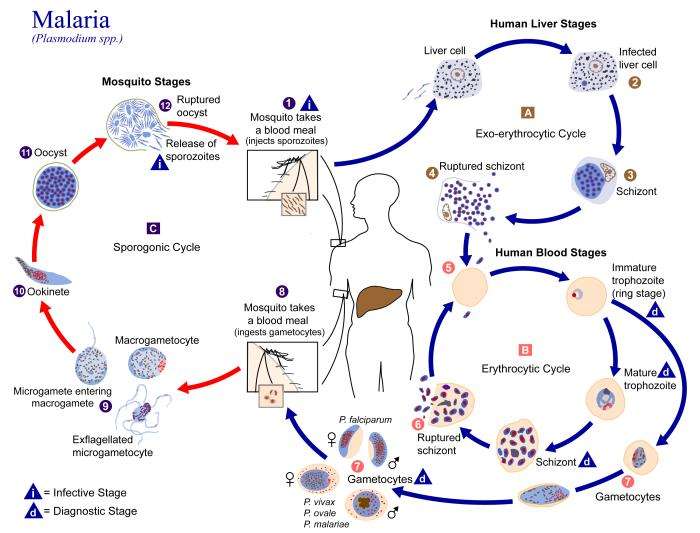
I. Asexual cycle in human host:
- Human gets infected with plasmodium falciparum by the bite of female Anaphelese mosquitoes or by inoculation of infected blood during transfusion or by congenital route from infected mother to child.
- In human hosts, two main stages of development is seen. They are;
- Pre-erythrocytic schizogony in liver
- Erythrocytic schizogony and gametogenesis in RBCs
i. Pre-erythrocytic or primary exo-erythrocytic schizogony:
- This comprises a single cycle and lasts for 6 days.
- Infected mosquitoes during bite inject sporozoites along with saliva into blood vessesls. These motile sporozoites are carried rapidly withon 30 minutes to the liver by blood stream.
- A protein called circumsporozoite protein covers the surface of sporozoite. It binds specifically and non-covalently with receptors present on the basolateral area of hepatocyte. Hence sporozoites enter into liver cell and not into any other cell in human host.
- Within liver cell, sporozoite undergoes a stage of asexual reproduction. During this cycle, sporozoite are transformed into trophozoites. The growing trophozoite feed on host cell cytoplasm.
- After few days, trophozoites mature and begins schizogony. Numerous daughter nuclei are first produced subsequently leading to the development of multinucleated liver stage schizonts (EE schizonts).
- These schizonts are spherical, multinucleated and measures 60µm or more in diameter. They contains 2000-5000 uninucleated merozoites.
- Mature EE schizonts and liver cell ruptures releasing thousands of merozoites into blood stream.
- Secondary exo-erythrocytic schizogony is absent in falciparum infection.
ii. Erythrocytic schizogony:
- Merozoites releasing from liver cell attach and invasion erythrocyte and begins erythrocytic schizogony.
- falciparum does not shows any special affinity for any particular type of RBC but invade both reticulocyte and erythrocyte (young and old).
- The merozoites become attached to the glycoprotein and other sialoprotein on surface of red cell.
- The nature of haemoglobin and red blood cell enzymes influences the development of merozoites inside RBCs. Development of falciparum is suppressed in presence of fetal haemoglobin and also in presence of other few haemoglobin.
- Indide RBc, merozoites develops into young trophozoites or ring form. They feed on haemoglobin by ingesting red cell cytoplasm.
- The trophozoites multiplies by mitosis to become mature schizonts.
- A mature schizont is less symmetrical and contains 8-32 merozoites and haemozoin. Rupture of schizonts release merozoites into blood circulation. These merozoites within second attach and penetrate new RBC and begins new erythrocytic schizogony.
- Erythrocytic schizogony is completed with 48 hours and always take place inside capillaries and vascular layer of internal organs. Therefore, in P. falciparum infection schizonts and merozoites are usually not demonstrated in peripheral blood smear preparation.
iii. Gametogenesis in RBC:
- After two or three erythrocytic schizogony, some of the merozoites instead of developing into schizonts, invade new erythrocyte and develop into male and female gametocytes.
- These gametocytes develops in RBCs of bone marrow and spleen.
- The specific stimulus for the production of gametocytes is not known. It is believed to be due to lack of nutrients, accumulation of metabolic or parasitic debris or due to development of immunity.
- The gametocytes are crescent shape with haemozoin granules found in the central part of cytoplasm surrounding the nucleus. Only mature gametocytes are found in peripheral blood.
- Gametogenesis completes in 96 hours.
II. Sexual cycle in definitive host mosquito:
iv. Sporogony:
- The process of formation of sporozoite is called sporogony.
- Anopheles mosquitoes during its blood meal from infected person, ingest both the sexual and asexual forms of parasite along with blood.
- Mature sexual form ie. Gametocytes are only capable of development, rest forms die and digested.
- It has been estimated that in order to infect a mosquito, the blood of human carrier must contain atleast 12 gametocytes per mm3 of blood and number of female gametocytes (macrogametocyte) must be in excess to male gametocytes.
-
i. Exflagellation:
- In the mid-gut of mosquito, the male gametocytes divides rapidly through a process of transformation known as exflagellation giving rise to 4-8 thread like filamentous structure, microgametes.
- An increase in pH caused by escape of CO2 from blood is suggested to be the stimulus for process of exfalgellation. A single microgametocyte gives rise to 6-8 microgametes.
- The macrogameocyte does not show any flagellation but mature by simple process of nuclear reduction and extension of polar bodies. A single macrogamete is formed from a single macrogametocyte.
-
ii. Formation of zygote:
- By the process of chemotaxis, microgamete are attracted towards macrogamete. One of the male gamete attaches to peripheral side of macrogamete and fertilize to form zygote within 20 minutes to 2 hours after blood meal by mosquitoes.
-
iii. Formation of Ookinete and Oocyst:
- In the next 24 hrs, the zygote lengthens and matures into Ookinete.
- Ookinete is 11-13 µm in length and 2.5 µm in width. It penetrates gut wall where it secrete a thin wall and grows into a spherical structure known as Oocyst.
- Oocyst is spherical 6-12 µm in diameter. It contains single nucleus and pigments granules. As Oocyst mature, it increases in diameter from 6µm to 60µm and meiosis and mitotic division follow to form large number of haploid sporozoites.
-
iv. Release of sporozoites:
- The oocyst ruptures, releasing sporozoites in the body cavity (haemocoel) of mosquito. The sporozoites are distributed through the circulating fluids into various organs and tissue of mosquito except ovaries.
- Sprozoites have special predilection towards salivary glands and ultimately reaches maximum concentration in the salivary duct.
- Sporogony completes in 9-10 days. The mosquitoes at this stage are infectious and a single bite can repeats the asexual cycle in human host.
-
Pathogenesis and pathology of Plasmodium falciparum:
Mode of transmission:
- Human are the only source of falciparum malaria. The infection is transmitted by;
- Bite of infected Anopheles mosquito harboring sporozoites
- Blood transfusion
- Transplacental transmission
- Organ transplantation
Virulence factors:
-
i. High level of parasitaemia:
- In P. falciparum malaria, parasite density exceeds more than 250,000-300,000/ml of blood due to invasion of erythrocytes of all ages.
- 30-40% of total RBCs are infected
-
ii. Sequestration of parasite:
- Sequestration is the condition of holding back of mature parasites in vital organs. It is exclusively shown by falciparum due to ability to cytoadherence.
- Inside RBC, P. falciparum merozoites produces a protein within erythrocyte surface membrane in the form of deformation called knobs. These knobs produce high molecular weight strain specific adhesive protein. These proteins in turn mediate attachment of parasite to receptors on endothelium of capillaries and veins. This causes sequestration of parasitized erythrocytes in the small post capillaries of internal vital organs especially CNS, kidney, spleen and lungs
-
Cytokines:
- falciparum produces a number of cytokines such as IL-1, TNF and IFN-Ƴ which are believed to contribute to end organ disease involving the kidney, lungs and brain.
-
Pathogenesis of disease progression:
- The clinical symptoms of malaria are primarily caused by the asexual intra eryhtrocytic stage of parasite. The disease is not caused either by sporozoites, developing stages of parasites in liver, merozoites releasesd from liver or by gametocytes.
- The diseaseprocess in malaria mainly occurs due to;
- The local and systemic response of host to parasite antigens
- Tissue hypoxia caused by reduced O2 delivery because of obstruction of blood flow by parasitized erythrocytes
- Anaemia caused by destruction of large number of red cells
- The pathological changes are seen primarily in spleen, bone marrow, liver, lungs, kidney and brain. The infected organs shows following common features;
- Pigments are present in various organs giving the characteristic slate-gray or black appearance
- The cells of reticuloendothelial system show hyperplasia
- Free pigments, free plasmodia and infected erythrocytes are present within capillaries of these organs. The capillaries also contains macrophages with infected RBCs and segmented plasmodia
- Sometimes thrombi caused by aggregation of pigments may also occur in capillaries.
Clinical manifestation and disease caused by Plasmodium falciparum:
- Infection with P. falciparum caused intermittent fever called malaria. The word malaria was derived from two Italian words ‘mala’ and ‘aria’ meaning bad air.
- falciparum causes falciparum malaria or malignant tertian malaria. It is also responsible for pernicious malaria.
- Incubation period is 10-14 days.
i. Falciparum malaria:
- Prodromal period:
- The prodromal period varies from a few days to several days. This period includes non-specific symptoms such as malaise, myalgia, headache and fatigue. Some localized symptoms such as chest pain, abdominal pain and arthralgia are also seen.
- Malarial paroxysm:
- It is the classical manifestation of acute malaria, characterized by fever, chill and rigor. It generally starts in afternoon but may starts in nay time.
- Each paroxysm shows a succession of 3 stages;
- Cold stage
- Hot stage
- Sweating stage
- Fever is the key clinical manifestation. Fever occurs every 48 hours which is irregular and does not shows any distinct periodicity pattern.
Anaemia:
- Anaemia is normochromic and normocytic. It is severe in falciparum infection.
- Lysis of parasitized and-non parasitized RBCs, suppression of erythropoiesis in bone marrow, increased clearance of non-parasitized RBCs by spleen and autoimmune response are the reason for anaemia
- Hepatosplenomegaly
- Uncomplicated malaria shows moderate splenomegaly and tender hepatomegaly or even reveal no abnormalities.
iii. Pernicious malaria:
- The term ‘pernicious malaria’ refers to a series of phenomenon occurring during course of an infection P. falciparum which, if not effectively treated threatens the life of patients within 1-3 days.
- Severe falciparum malaria may develops into serious complication called pernicious malaria as a result of capillary blockage.
- Complication occurs in non-immune person, immune-compromised person, pregnant woman and person with splenectomy.
- Various manifestation of pernicious malaria are;
- Cerebral malaria: hyperpyrexia, coma, paralysis
- Algid malaria; cold and clammy skin with peripheral circulatory failure
- Septicaemic malaria: high temperature, bilious remittent fever, pneumonia, cardiac syncope
iv. Black water fever:
- It is a manifestation of falciparum malaria occurring in previously infected individuals and is characterized by sudden intravascular hemolysis followed by fever and haemoglobinuria.
- The symptoms is known as black water fever due to dark red to brown-black appearance of urine because urine consists of free haemoglobin.
- An autoimmune mechanism has been suggested in pathogenesis of black water fever. Eryhtrocytic autoantibodies produced in previous falciparum infection probably combine with auto-antigen (infected RBCs) occurring in new infection of erythrocytes with same strain of P. falciparum resulting in haemolysis of RBCs.
- Clinically this condition is manifests as high fever, vomiting, pain in loin, jaundice, haemoglobinaemia, haemoglobinuria, circulatory collapse and renal failure.
v. Cerebral malaria:
- The symptoms of cerebral malaria is caused by stagnant hypoxia due to adherence of Parasitized RBC to endothelium of cerebral venules and capillaries.
- Cerebral malaria is marked by severe headache, high fever, convulsion, changes in mental status and coma. Death may occurs within few hours
vi. Tropical splenomegaly syndrome (TSS):
- It is also known as hyper reactive malarial spenomegaly. It occurs in some patients living in endemic areas of Africa, Indonesia and New Guinea.
- TSS is characterized by massive splenomegaly, a moderately enlarged liver with hepatic sinusoidal lymphocytosis and a marked elevated serum IgM malarial antibodies.
- It is also characterized by absence of malarial parasites in peripheral blood.
- Clinical symptoms includes abdominal mass, dragging sensation of abdomen and sharp abdominal pain.
- Pulmonary oedema:
- This is the most serious complication of falciparum malaria
vii. Renal failure
viii. Hypoglycaemia with lactic acidosis:
- This condition is associated with quinine treatment.
- Hypoglycaemia results from the reduced glucose supply by impaired hepatic glycogenolysis and gluconeogenesis and increases consumption of glucose by parasite.
viii. Recrudescence:
- It refers to the occurrence of clinical malaria following the previous attack of falciparum malaria. It occurs due to persistence of small number of viable merozoites inside RBC in internal organs.
- It is believed to be due to inadequate treatment and frequently seen in drug resistant case, immune-suppressed and pregnancy.
- It occurs within a few weeks to months of previous attacks.
- Latent malaria:
- It refers to a state of asymptomatic malaria harboring plasmodium gametocytes in peripheral blood.
- These persons are reservoir of malaria and infectious to mosquitoes/
- Other complication:
- Septicaemia, aspiration pneumonia, gastro-intestinal bleeding, diarrhea, secondary bacterial infection etc.