
Enterobius vermicularis
- Enterobius vermicularis is commonly called the thread worm, pin or seat worm. It causes an intestinal parasitic infection called enterobiasis (anal itching) that occurs commonly in children.
Habitat:
- Adult worm (gravid females) live in the caecum and vermiform appendix of human, where they remain until the eggs are developed. They generally remain on the surface of the mucosa and may occasionally encyst in the submucosa layer.
Morphology:
- The adult worm is small, white in color, more or less spindle shaped and resembles a short piece of thread.
- They are visible to the naked eye.
- True buccal capsule is absent.
- A pair of cervical alae (wing like expansions) is present as the anterior extremity.
- The posterior end of the oesophagus is dilated into a conspicuous globular bulb/ a double- bulb oesophagus which is a characteristic feature of this nematode.
- The oral end has three lips with a dorso-ventral bladder like expansion of the cuticle.
Male worm:
- An adult male measures 2-4mm in length and 0.1-0.2mm breadth.
- The posterior third of the body is curved, sharply shortened and possess a exposed terminal copulatory spicule.
- The male worm dies immediately after fertilizing the females, therefore are rarely seen.
Female worm:
- Adult female is longer, 8-12mm in length and 0.3-0.5 mm in breadth.
- The posterior end is extremely straight and drawn out into a long, tapering and finely pointed tail, which is 1/3rd the length of the worm.
- The female reproductive organs are paired and T-shaped.
- A large number of eggs with an average of 11,105 eggs are present in the uterus of the gravid female that fill up the entire body of the female worm.
- The gravid female dies within 2-3 weeks after laying eggs.
Eggs:
- The embryonated eggs are infective to human.
- The eggs are colorless, measuring 50-60 µm in length and 20-32µ m in breadth.
- They are typically plane convex, with one flattened side and one convex side.
- The eggs are surrounded by a thin, hyaline, transparent shell composed of 2 layers of chitin.
- Egg contains a coiled tadpole like larva.
- Egg can floats in saturated salt solution.
- The egg become infective after exposure to atmospheric oxygen for 6 hours and is more resistant to antiseptics.
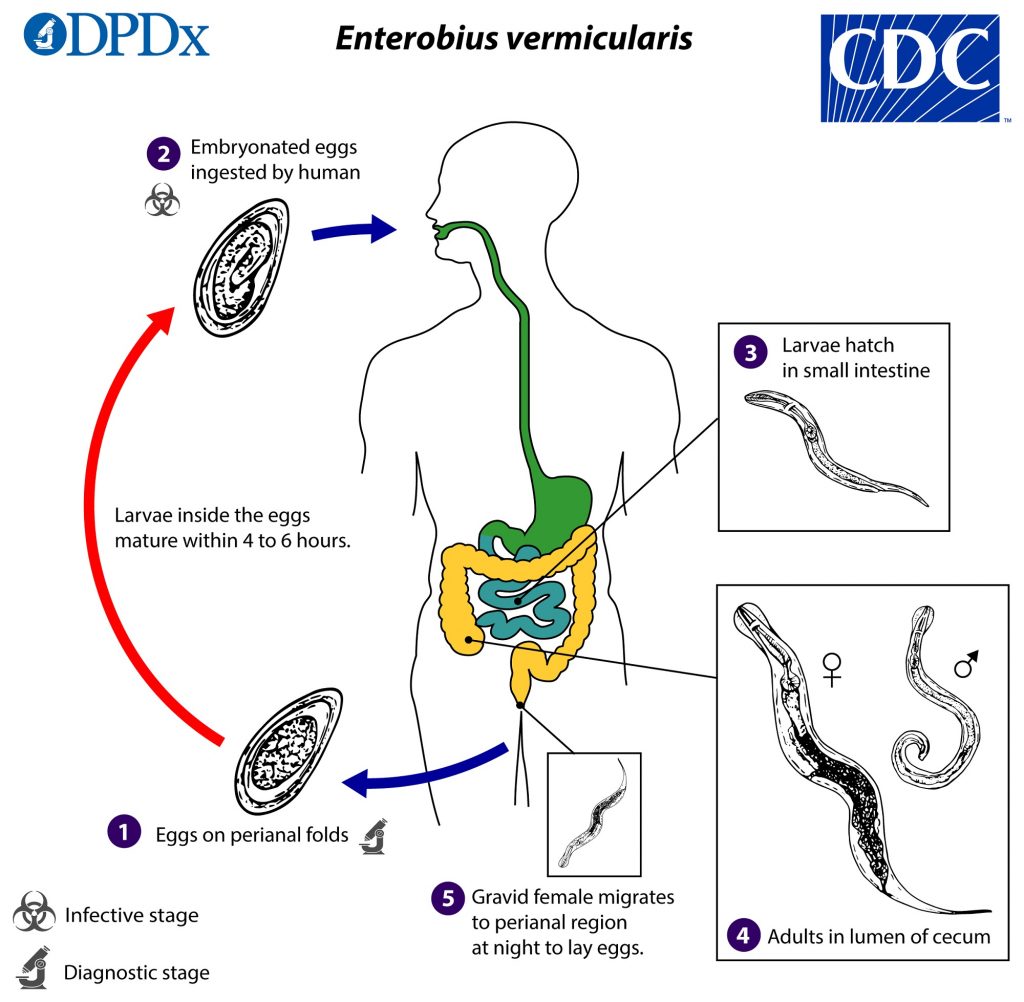
Life cycle of Enterobius vermicularis:
- The life cycle of E. vermicularis is simple and is completed in single host (Human host).
- No intermediate host is required.
- Human acquires infection by ingestion of the embryonated eggs attached to their nails during scratching of the perianal area.
- The egg shells are dissolved by digestive juices and the larva escape in the small intestine than they migrate to the caecum and vermiform appendix, where they develop to adult worms within 15-30 days of infection.
- Female worms may produce a pheromone to attract males.
- The male worm coils around a female worm with its curved area over the female genital pore.
- Male use spicules to hold female during copulation. The male dies immediately after fertilizing the female.
- The gravid female then migrates to the perianal skins at night, stimulated by a drop in body temperature of the host.
- It will only lays eggs on the perineum, because air acts as stimulant for laying eggs.
- The ejection of eggs is so forceful that the eggs can be spread out over the perianal area.
- After oviposition the female often dies.
- Eggs trapped in perianal folds may hatch out the larva and may enter intestine directly via the anus. This process is known as retro-infection.
- Occasionally larva may enter the vulva and infect the vagina of women.
- Whole life-cycle completes within in 2-13 weeks.
Mode of transmission:
- Infected human beings are the only source of infection. No extra human reservoir is known.
- It is primarily a disease of children and intra-family transmission is very common.
- The different modes of transmission are-
- Ingestion of eggs due to contaminated fingers, commonly seen in children.
- Handling contaminated night clothes of the children.
- Inhalation of air-borne eggs present in the dust.
- Retro infection, occasionally seen mainly in adults.
Pathogenesis:
Pathogenicity of eggs:
- Significant pathological lesion are caused by the eggs.
- The eggs adhere well on surface of the skin and by thin natural perianal or perianal itching.
Pathogenicity of adult worms:
- Adult worms attach to the mucosa and feed on intestinal content, bacteria and possibly epithelial cells, causing minute ulceration which may lead to mild catarrhal inflammation with diarrhea, eosinophilia and bacterial infection.
- Infection are characterized by intense perianal itching.
- Patients vigorously scratch themselves attempting to relieve the itching and doing so often cause skin damage, bleeding, bacterial infection and intensified itching
- Allergic reaction in the sensitized hosts is observed due to absorption of metabolites secreted by the worm.
Clinical manifestation: Diseases
- Most patients are asymptomatic.
- In symptomatic patients, the most common complaint is perianal and perianal pruritus, usually nocturnal or in the early morning.
- Other complaints include abdominal pain, irritability and restlessness.
- Heavy infection in children may cause anorexia, behavioral changes such as sleep disturbance, nausea, nail bite, grinding teeth at night.
Complications: Urethritis, Endomeritis, Appendicitis
Epidemiology and geographical distribution:
- The nematode is cosmopolitan, found all over the world.
- Unlike many other parasite disease, the incidence is higher in developed countries and in temperate climate than in tropical countries.
- Rate of infection is highest in children.
- Infection found more in whites than in blacks, which may be due to racial immunity.
Laboratory diagnosis:
- Eggs are rarely found in faeces, so conventional stool sample examination techniques are not useful.
- Infection are best diagnosed by microscope detection of adult worms or microscopic detection of eggs on the perineum.
- Detection of adult worms
- Motile worms may be seen perianal skin shining under bright light when close visual examination are conducted during night or early in the morning.
- Adult worms may sometimes be observed on the surface of fresh stool samples, during garments, perianal folds.
- Detection of eggs
- Microscopic demonstration of characteristic eggs in the perianal scrapings is the method of choice for the diagnosis of enterobiasis
- Anal or perianal specimens can be collected by NIH swab, cellophane swab or scotch tape swab method.
- Scotch tape swab method is a simple and effective procedure. In this procedure transparent adhesive tape is pressed firmly against perianal skin and then spread on to a microscope and observed for pinworm eggs.
- The perianal specimens are best collected in the morning before the child goes to the toilet and takes bath.
- At least 3 scotch tape swab should be collected for 3 consecutive days to rule out E. vermicularis infection.
- Since anal itching is a common symptom of pinworm, the third option for diagnosis is analyzing samples from under fingernails under microscope.
Treatment
- Pyrantel pamoate is the drug of choice
- Single dose
- Oral administration
- 5 mg/kg single dose
- Mebendazole is also effective
- Others drug are- albendazole, piperazine, pyminium pamote
Prevention and control
- Keeping finger nails short
- Frequent hand washing before meals and after defecation
- Good personal hygiene.
- Treatment of infected case and all other members in the family or institution.
- Fingers should not be put in mouth as habit.
- Washing the bed liners and night dress daily.