
Hemostasis mechanism of preventing blood loss
- One drawback of a circulatory system such as ours, in which the liquid blood is under high pressure, is that serious bleeding can take place after even a slight injury.
- To prevent the possibility of uncontrolled bleeding, we have a three-part hemostatic mechanism consisting of:
- The constriction of blood vessels
- The clumping together (aggregation) of platelets
- Blood clotting
- Overall, hemostasis is a specific type of homeostasis that prevents blood loss.
1. Vasoconstrictive phase:
- Normally, when a tissue is damaged and blood escapes from a blood vessel, the vessel wall constricts in order to narrow the opening of the vessel and slow the flow of blood.
- This vasoconstriction is due to contraction of the smooth muscle of the vessel wall as a direct result of the injury and the release of vasoconstrictor chemicals from platelets.
- Proper vasoconstriction is also enhanced by pain reflexes, producing constriction in proportion to the extent of the injury.
- Constriction of capillaries, which donot have muscular layers, is due to the vascular compression caused by the pressure of lost blood that accumulates in surrounding tissues.
- Injured blood vessels may continue to constrict for 20 min or more.
2. Platelet phase:
- The next event in hemostasis is the escape from blood vessels of platelets, which swell and adhere to the collagen in adjacent connective tissues.
- This attachment stimulates vasoconstriction.
- By now, the platelets have become very sticky, so that as more and more of them move into the injured are they stick together.
- In about a minute they can clog a small opening in the vessel with a platelet plug.
- The process is called platelet aggregation.
- It is important partly because it successfully stops hundreds of small hemorrhages every day and partly because it triggers the blood-clotting mechanism.
3. Coagulation phase: Basic mechanism of blood clotting
- If the blood vessel damage is so extensive that the platelet plug cannot stop the bleeding, the complicated process of blood clotting- the coagulation phase- begins.
- The basic clotting mechanism involves the following events:
- Supported by a plasma globulin called antihemophilic factor (AHF), blood platelets disintegrate and release the enzyme thromboplastinogenase and platelet factor 3.
- Thromboplastinogenase combines with AHF to convert the plasma globulin thromboplastinogen into the enzyme thromboplastin.
- Thromboplastin combines with calcium ions to convert the inactive plasma protein prothrombin into the active enzyme thrombin.
- Thrombin acts as a catalyst to convert the soluble plasma protein fibrinogen (‘giving birth to fibrin’) into the insoluble, stringy plasma protein fibrin.
- The fibrin threads entangle the blood cells and create a clot.
- The basic process may be summarized as follows:
- Thromboplastinogen —–Thromboplastinogenase+ antihemophilic factor——-> Thromboplastin
- Prothrombin ——-Thromboplastin+ calcium ions-——-> Thrombin
- Fibrinogen ——thrombin————> Fibrin
List of Blood clotting factors:
| Coagulation factors number and name | Description and origin | Function |
| Plasma coagulation factors: | ||
| factor I: Fibrinogen | Plasma protein synthesized in liver. | Precursor of fibrin, converted to fibrin in final stage of clotting. Serum is plasma minus fibrinogen. |
| factor II: Prothrombin | Plasma protein synthesized in liver. Synthesis requires vitamin K. | Precursor of thrombin, the enzyme that converts fibrinogen into fibrin. |
| factor III: Thromboplastin | Complex lipoprotein formed from disintegrating platelets or tissues. | Combines with calcium to convert prothrombin into active thrombin. |
| factor IV: Calcium ions | Inorganic ion in plasma, acquired from bones and diet. | Essential for formation of thrombin and for all stages of clotting |
| factor V: Proaccelerin, labile factor, or accelerator globulin | Plasma protein synthesized in liver. | Necessary for extrinsic and intrinsic pathways |
| factor VI | No longer thought to be a separate entity, possibly the same as factor V. | |
| factor VII: Serum prothrombin conversion accelerator (SPCA), stable factor or proconvertin | Plasma protein synthesized in liver. Synthesis requires vitamin K. | Necessary for first phase of extrinsic pathway. |
| facor VIII: Antihemophilic factor (AHF), antihemophilic factor A, or antihemolytic globulin (AHG) | Plasma protein synthesized in liver and other tissues. | Necessary for first phase of intrinsic pathway. Deficiency causes hemophilia A, genetic disorder |
| factor IX: Plasma thromboplastin component (PTC), Christmas factor, or antihemophilic factor B | Plasma protein synthesized in liver. Synthesis requires vitamin K. | Necessary for first phase of intrinsic pathway. Deficiency causes hemophilia B. |
| factor X: Stuart-Prower factor or Stuart factor | Plasma protein synthesized in liver. Synthesis requires vitamin K. | Necessary for early phases of extrinsic and intrinsic pathways. |
| factor XI: Plasma thromboplastin antecendent (PTA) or antihemophilic factor C | Plasma protein synthesized in liver. | Necessary for first phase of intrinsic pathway. Deficiency causes hemophilia C. |
| factor XII: Hageman factor or glass factor | Plasma protein, source unknown. | Necessary for first phase of intrinsic pathway, activates plasmin, activated by contact with glass, probably involved with clotting outside body. |
| factor XIII: Fibrin-stabilizing factor (FSF) or Larki-Lorand factor | Protein present in plasma and platelets, source unknown. | Necessary for final phase of clotting. |
Platelet coagulation factors:
| Pf1: Platelet factor 1 or platelet accelerator | Platelets | Same as factor V, accelerates action of platelets. |
| Pf2: Platelet factor 2 or thrombin accelerator | Platelets, phospholipid. | Accelerates thrombin formation at start of intrinsic pathway, accelerates conversion of fibrinogen into fibrin. |
| Pf3: Platelet factor 3 or platelet thromboplastic accelerator | Platelets, phospholipid. | Necessary for first phase of intrinsic pathway. |
| Pf4: Platelet factor 4 | Platelets | Binds the anti-coagulant heparin during clotting. |
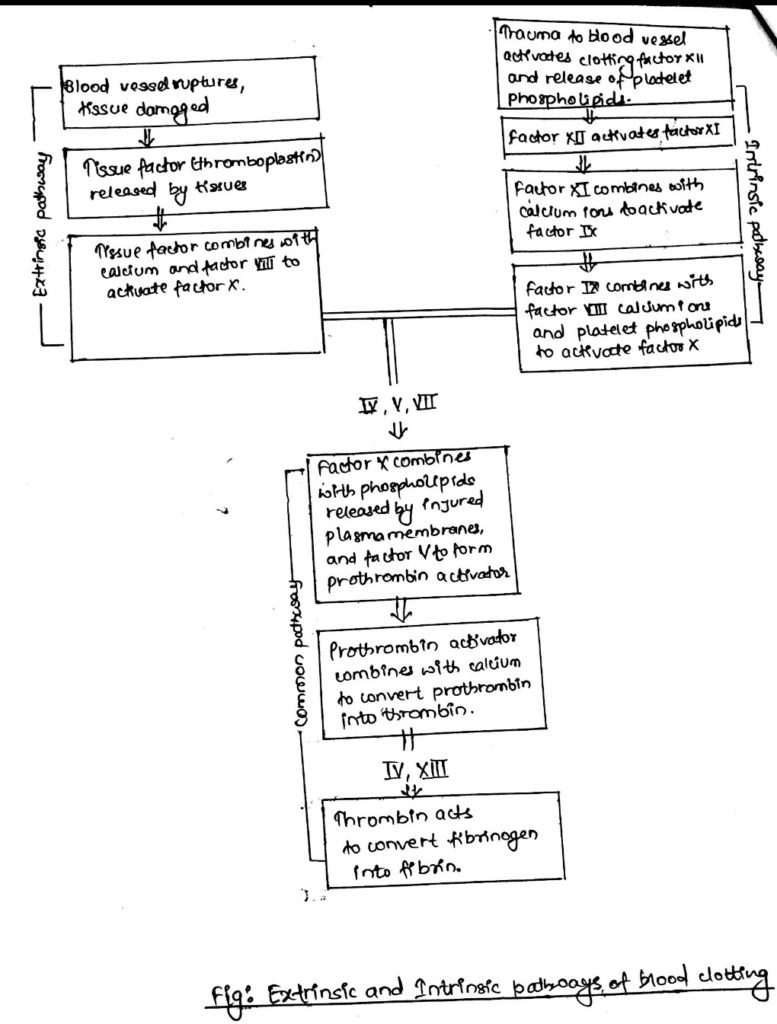
Extrinsic and intrinsic pathways:
- Two partially independent pathways were identified in 1960s for the triggering of a blood clot:
- The extrinsic pathway is a rapid clotting system activated when blood vessels are ruptured and tissues are damaged.
- The intrinsic pathway is activated when the inner walls of blood vessels become damaged or irregular.
- Damaged tissue triggers the extrinsic pathway, which initiates blood clotting by the release of thromboplastin, known in this form as tissue factor. (A somewhat different form of thromboplastin is at work at the site of ruptured vessels, triggered by the disintegration of platelets).
- Tissue factor combines with a mixture of enzymes and the phospholipids from damaged cell membranes released by the injured tissue to produce a substance called pro-thrombin activator.
- At this point, the extrinsic system merges with the intrinsic system to activate yet another mechanism (called the common pathway) that actually produces the clot.
- The common pathway includes steps 3, 4, and 5 described above.
- The intrinsic pathway for initiating blood clotting uses only substances found in the blood.
- These substances are called clotting factors.
- Injury to the inner wall of a blood vessel activates clotting factor XII, which triggers a series of rapid chemical reactions usually called the ‘cascade effect’.
- Each step activates the next step in the sequence until prothrombin activator is produced.
- After prothrombin activator is formed in the extrinsic and intrinsic pathways, the basic blood-clotting process proceeds through the common pathway.
- The extrinsic pathway usually produces a clot in as little as 15 sec, while the intrinsic pathway requires 2 to 6 min.
- At this point, the fibrin threads form only a weak mesh, and the clot must be strengthened if it is to hold.
- Platelets and plasmaglobulins release a fibrin-stabilizing factor that responds to thrombin to create an interlacing pattern of fibrin threads.
- Within a few minutes after the clot is formed, it begins to contract, squeezing out serum and helping the clot solidify.
- The power to contract comes from platelets, which contain actin and myosin, the same proteins that make muscle contraction possible.
- Platelets contain more actin and myosin than any tissue in the body except muscle.
- Most of the serum is drained within an hour, and the solid clot is finally complete.
- A ‘scab’ forms, dries up, and in a few days falls off as the underlying tissue heals.
- A well-known dietary substance involved with blood clotting is vitamin K.
- It is found in leafy green vegetables, tomatoes, vegetable oils and also produced by intestinal bacteria, vitamin K is necessary for the production of prothrombin and other clotting factors by the liver.
Blood clotting inhibitors
i. Anticoagulant:
- As many as 35 compounds may be required for blood coagulation.
- Such a complex system of checks and balances is necessary to prevent clotting when there is no bleeding.
- An unwanted clot in a blood vessel that cuts off the blood supply to a vital organ is one of the body’s worst enemies.
- Most of the body’s anticoagulant substances circulate within the blood, and the blood vessels themselves help prevent clotting.
- The blood vessels contribute in two ways.
- First, the smoothness of the inner walls normally prevents activation of the intrinsic clotting mechanism.
- Second, a thin layer of negatively charged protein molecules attached to the inner walls repels the clotting factors, preventing the initiation of clotting.
- Injury to a blood vessel removes both of these safeguards.
- The rough damaged wall of the vessel and the negatively charged collagen layer beneath the smooth endothelium initiate the platelet phase of hemostasis.
- If the platelet plug that forms cannot stop the loss of blood, factor XII is activated, along with the rest of the intrinsic pathway.
ii. Heparin and antithrombin:
- One of the most powerful anticoagulants in the blood is heparin, a polysaccharide produced by mast cells and basophils.
- Heparin is concentrated mostly in the liver and lungs.
- Minute quantities of heparin in normal circulating blood also prevent clotting by combining with the antithrombin-heparin cofactor (also called antithrombin or antithrombin III) to induce the co-factor to combine with thrombin 1000 times more rapidly than usual.
- Such a rapid binding to thrombin removes it almost instantly from the bloodstream and makes clotting almost impossible.
- Without heparin, antithrombin-heparin cofactor binds to thrombin molecule for molecule, removing it from the blood in about 15min.
- The combination of heparin and antithrombin-heparin cofactor also reacts with several clotting factors in the extrinsic and intrinsic pathways, further inhibiting blood clotting.
- Thrombin itself acts as an anticoagulant.
- When its concentration becomes too high, it destroys factor VIII to prevent clotting.
iii. Fibrinolysis by plasmin:
- Clot prevention is important, but so is clot destruction, or fibrinolysis (‘fibrin breaking’).
- Small blood clots form continually in blood vessels throughout the body.
- If they are not removed promptly, the blood vessels become clogged.
- In the process of fibrinolysis, a blood protein called plasminogen is activated into an enzyme called plasmin.
- The plasmin digests the threads of fibrin by first making them soluble and then breaking them into small fragments.
- The fragments are removed from the bloodstream by phagocytic white blood cells and macrophages.
- Excessive amounts of coagulants are routinely removed by the liver.
Anticoagulant drugs:
- When used under medical supervision, anticoagulant drugs can sometimes remove blood clots in the body.
- The best-known anticoagulant drug is aspirin (acetylsalicylic acid), which works by preventing platelets from sticking together to form a plug.
- It also inhibits the release of clot-promoting substances from platelets.
- One drug that digests the fibrin threads of a clot is streptokinase, which is released by certain streptococcal bacteria.
- Streptokinase activates plasminogen to speed fibrinolysis.
- It is used to dissolve blood clots (thrombi) in veins and arteries.
- Streptokinase also helps dissolve the fibrin threads in a blood clot by converting plasminogen into plasmin, the fibrin-destroying enzyme.
- Genetically engineered (recombinant) tissue-plasminogen activator (rt-PA) is effective in dissolving intravascular blood clots when delivered directly to a clotted area through a catheter.
- For example, if rt. PA is used within the first several hours after a blood clot forms in a coronary artery, the heart is often spared a serious damage.
- When vitamin K is in short supply, the liver produces enough prothrombin and other clotting substances for normal clotting.
- Dicumarol is a compound that resembles vitamin K to such an extent that the liver enzymes that form prothrombin will pick up dicumarol instead of vitamin K.
- The anti-coagulatory effect of dicumarol is often used to prevent clotting after surgery.
- In addition to being used to remove blood clots and keep blood from coagulating during surgery, anti-coagulant drugs may be necessary to prevent clotting in blood that will be used later for blood transfusions.
- To avoid such clotting, a dilute sterile solution of a citrate or an oxalate salt is added to collected blood.
- Clotting doesnot occur because citrate ions or oxalate ions combine with the available calcium ions, making calcium unavailable for its usual blood-clotting functions.
Blood coagulation tests:
- Several tests are used to determine blood-clotting time.
- The most popular ones are platelet count, bleeding time, clotting time, and prothrombin time.
- The blood platelet count must be greater than 150,000 per cubic millimeter in order for normal coagulation to take place.
- Also, if platelet function is not normal, normal coagulation may not occur.
- A pierced fingertip or earlobe usually bleeds for 3 to 6 min.
- A longer bleeding time for this wound generally indicates a platelet deficiency.
- Clotting time is determined by placing blood in a test tube and tipping it back and forth every 30sec or until it clots.
- This usually occurs in 5 to 8 min.
- Because the condition and size of test tubes vary, standardization is necessary to obtain accurate results.
- The test for prothrombin time (PT) indicates the amount of prothrombin in the blood.
- Immediately after blood is removed, oxalate is added to prevent the prothrombin from being converted into thrombin.
- Then calcium ions and tissue extract containing thromboplastin are added to the blood.
- The calcium offsets the effect of the oxalate, and the tissue extract activates the conversion of prothrombin.
- The time usually required for blood to clot, referred to as the prothrombin time, is about 12 sec.
- A longer prothrombin times also mean a decreased quantity of some factor other than prothrombin.
- Similar tests are used to determine the relative quantities of other clotting factors.